
What is Ovarian Reserve?
Ovarian reserve is a phrase that is commonly used to possibly indicate the fertility status of a female. It technically predicts the quality and the quantity of potentially fertile eggs that the ovary is capable of producing.
A good ovarian reserve does not guarantee fertility or conception. Ovarian reserve is only one of the many factors that are responsible for infertility. On the same note, a poor ovarian reserve does not mean that one will be infertile. It is merely a predictor.
What is Ovarian reserve testing?
Ovarian reserve testing (fertility testing) is a catch all term used nowadays to include lab and ultrasound testing that might predict fertility. The total number of gonadotropin (hormone)-responsive follicles (see below) and oocytes (premature eggs) contained within an individual’s ovaries at any given time is known as her “ovarian reserve”. Simply stated, follicles are immature eggs in the ovaries that if stimulated by the correct hormones within a female body will develop into a mature egg.
Why does Ovarian reserve matter?
When a female fetus develops within a womb, its reproductive organs start to produce oocytes. This starts as early as 12 weeks of pregnancy. Oocytes are simply the little building blocks which eventually have the potential to develop into an egg. Note that not all oocytes end up becoming eggs, just like not all the sperms end being used to fertilize the egg.
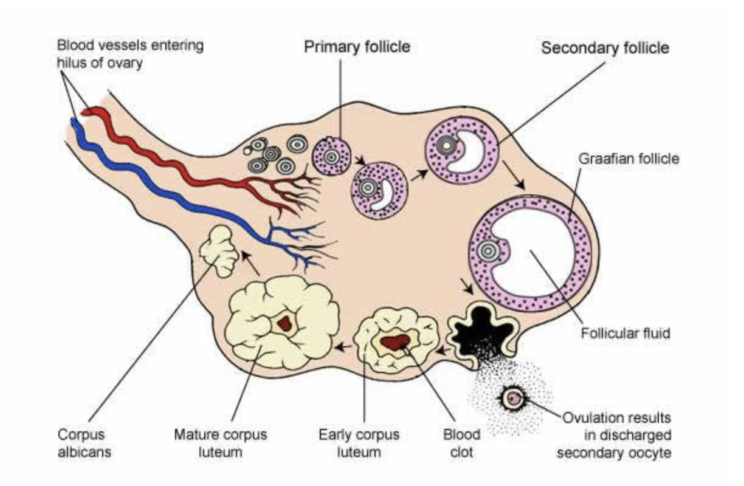
A female fetus has the maximum number of oocytes at 20 weeks of pregnancy. From that point on, there is loss of oocytes (pre-eggs) until there are approximately 500,000 oocytes left at puberty. From there on, every month a group of follicles gets activated. These follicles or building blocks can either progress to a dominant follicle leading to ovulation or shrink and eventually die.
If a pregnancy is achieved then the oocyte from the dominant follicle gets fertilized and progresses to a pregnancy.
What leads to a low Ovarian reserve?
Am I fertile? How can I get my fertility testing done? This is a common question we get all the time.
There are many reasons that might contribute to a low ovarian reserve. Below are some factors that might contribute to a low reserve. There could be many more that we don’t know of.
- Increasing age (> 35 yrs)
- Smoking
- Fragile X syndrome (FMR1 premutation)
- Turner’s syndrome (XO, mosaicism)
- Conditions causing ovarian injury e.g. extensive endometriosis (ovarian) surgery or pelvic infections.
- Autoimmune oophoritis
- Oophorectomy (removal of ovaries)
- Pelvic irradiation (radiotherapy)
- Chemotherapeutic drugs
- Idiopathic (unknown)
How can we test for Ovarian reserve?
As of now we can use a combination of certain blood test markers and ultrasound done in the right time of the cycle to predict the ovarian reserve. This is a continuously evolving field and new discoveries might lead to a more accurate predictive model.
Which hormones or markers are being used at this time?
- AMH – Antimullerian Hormone
- FSH – Follicle Stimulating Hormone
- Estradiol – Estrogen (E2)
- Inhibin B
Let’s discuss each of these below:
AMH testing
Antimüllerian hormone (AMH) is produced by the granulosa cells (ovarian cells) surrounding each oocyte in the developing ovarian follicle. AMH is secreted primarily by the preantral and small (less than 8 mm) antral follicles of the ovary. These follicle numbers slowly decline with age. Therefore, AMH levels also slowly decline with age and are reflective of ovarian reserve at a given time.
FSH
FSH stands for Follicle Stimulating Hormone. As the name suggests, it stimulates the ovarian follicles. It is produced by the pituitary gland in the brain. The FSH levels fluctuate throughout a woman’s lifecycle even before birth. The levels change not only daily or monthly but also have varying pulses throughout the day.
What controls FSH changes is a complex mechanism, much of it is still being studied. As of now, we know that as women approach menopause, the FSH levels start to creep up and the ovaries become less responsive to the stimulation by FSH.
Estradiol
Estradiol (E2) is one of the three types of estrogens found in the body. E2 is the main estrogen responsible for the female reproductive functions. The other two types of Estrogens are Estrone (E1) and Estriol (E3).
Estradiol is produced by the Granulosa cells of the ovary, the production of which is stimulated by FSH secreted by the pituitary.
The secretion of both FSH and Estradiol is pulsatile. Serum FSH levels (> 15-20 IU if elevated on Day 3 of cycle (early follicular phase) indicate menopausal status. Serum Estradiol levels below 35-50 pg/ ml in the same time frame also might reflect lack of active follicles producing estradiol. However, FSH and Estradiol levels can only be supportive evidence and should not be used as sole indicators for ovarian reserve since these levels can vary depending on age, PCOS, hormonal contraceptive usage, presence of irregular periods and ovarian dysfunction due to other causes.
Very commonly a woman may be misdiagnosed with low reserve or premature menopause if the testing of the above two hormones is done at the wrong time of the cycle.
What are some of the benefits of testing AMH?
Advantages of AMH over other tests include:
- Can be done at any time in the menstrual cycle.
- Not affected by hormonal contraceptives or other medications.
- Not influenced by irregular periods or conditions such as PCOS.
- It is a known predictor of ovarian response to exogenous gonadotropin stimulation in infertile women undergoing assisted reproduction cycles
What are some caveats of AMH testing?
- AMH cannot be reliably used as an indicator of “fertility” status in women not seeking fertility treatment.
- It is not an indicator of risk of miscarriage.
- It is not predictive of PCOS
- It is not recommended to be used as a marker of peri-menopause or menopause.
What is the role of Inhibin B?
Inhibin B is another hormone produced by the ovarian cells. Inhibin B levels vary with menstrual cycle.
Inhibin B levels start to decline within 5 years of menopause. They have not been shown to be a reliable predictor of ovarian reserve. Low Day 3 (<45 pg/ ml) levels might indicate perimenopause but no standardized predictive levels have been developed.
What is the currently recommended regimen for Ovarian reserve testing?
Blood work: AMH (Anti Mullerian Hormone), FSH and Serum Estradiol on Day 3 of menstrual cycle.
Ultrasound: Transvaginal ultrasound evaluation of ovarian volume and count of follicles on Day 3 of menstrual cycle.
Does my insurance cover Ovarian reserve testing?
Unfortunately, most insurances do not cover ovarian reserve testing. Your insurance might cover a portion of your blood work or the initial counseling visit. The ultrasound will most likely not be covered. Best is to call your insurance company directly and give them the CPT codes.
How can I get my Ovarian reserve testing at Walk In Gyn Care?
We have designed two options for our patients to test for Ovarian reserve. Please note that this does not include a full infertility evaluation in case you are actively trying to get pregnant. That is a multi-step comprehensive process.
1st visit: Provider consult (annual or problem visit) and referral for Ovarian reserve testing. (we will bill your insurance as appropriate).
2nd visit: Day 3 blood work + Follicle count sonogram (Self pay: $300. We will not bill insurance).
3rd visit: Follow up for results discussion (can be in-person or tele visit). We will bill insurance as appropriate.
Total package $700.
This does not include the lab charges for the blood work. You will be billed directly by the lab.
How many visits will I need for Ovarian reserve testing?
- Initial Visit: Initial consult
- Testing schedule and fees as below:
Day 3 (Day 1 of menstrual cycle is the first day of bleeding)
BLOOD WORK
- Day 3
- FSH
- ESTRADIOL
- AMH – indicates Oocyte Quantity not quality.
ULTRASOUND (AFC)
- ANTRAL FOLLICLE COUNT
- Follow up visit: Results discussion.
What do the results mean?
Here is a concise summary of the currently used levels of each test marker. This has been compiled as a reference from standard resources. Again, remember that “fertility testing” is only a catch all phrase and can be a misnomer. Below are only guidelines and not to be taken as a be-all and end-all for your fertility status.
The interpretation of the test results can be very tricky and complicated. We strongly recommend that the interpretation be done after consultation with your gynecologist or infertility specialist. We also stress that the levels do not indicate a guaranteed pregnancy or definitely deem you as “infertile”. Just like the human body, we are all in a state of flux and live along a pendulum. Please do not rely on these levels as your sole indicator for the ability to conceive.
If you have any further questions, please feel free to schedule an appointment or just walk in.
Be safe, be strong and be prepared.
Dr. Adeeti Gupta
APPENDIX A: INTERPRETATION OF RESULTS
Interpretation of AMH
AMH <0.5 ng/mL: predicts reduced ovarian reserve with less than three follicles in an IVF cycle.
AMH <1.0 ng/mL: predicts baseline ovarian reserve with a likelihood of limited eggs at retrieval.
AMH >1.0 ng/mL but <3.5 ng/mL: suggests a good response to stimulation.
AMH >3.5 ng/mL: predicts a vigorous response to ovarian stimulation and caution should be exercised in order to avoid ovarian hyperstimulation syndrome.
Interpretation of AFC (Antral Follicle Count)
MORE THAN 7 – good.
Ideal: 7-10
Less than 5: Indicative of reduced response to fertility treatments.
5-10: 7 follicles are considered ideal.
More than 10: Risk of ovarian hyperstimulation with ovulation induction agents.
Best predictors are AMH and Antral Follicle Count.
Interpretation of FSH and Estradiol levels
FSH > 20 IU
ESTRADIOL <50 ***
>May indicate perimenopausal or postmenopausal status.**
FSH : 10- 20 IU
ESTRADIOL > 50
>>May indicate perimenopausal status or poor response to ovarian stimulation
FSH < 10 IU
Estradiol : 25- 50 IU
AMH : 0.5- 3.5
>>> Indicates that patient is not in menopause and has good ovarian reserve.
**If patient is menopausal (no period for 1 year then this can be done at any time).
**If patient has irregular periods, then the test should be done on Day 3 of cycle.
**If patient has scanty periods and is skipping cycles, then attempt should be made to repeat the test in 3 months.
**The tests are not to be used as an indicator of peri-menopausal or menopausal status if the patient is on any hormonal contraception or HRT.
**** Estradiol > 100 mg/dl- High risk of hyperstimulation with Clomiphene.
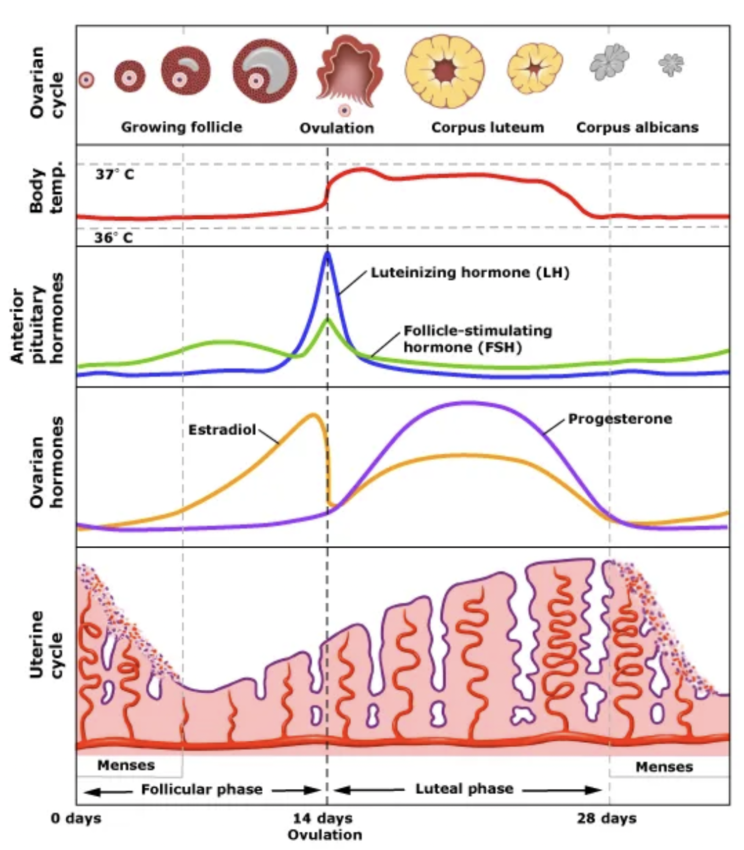
APPENDIX B: Ovulation in relation to hormones
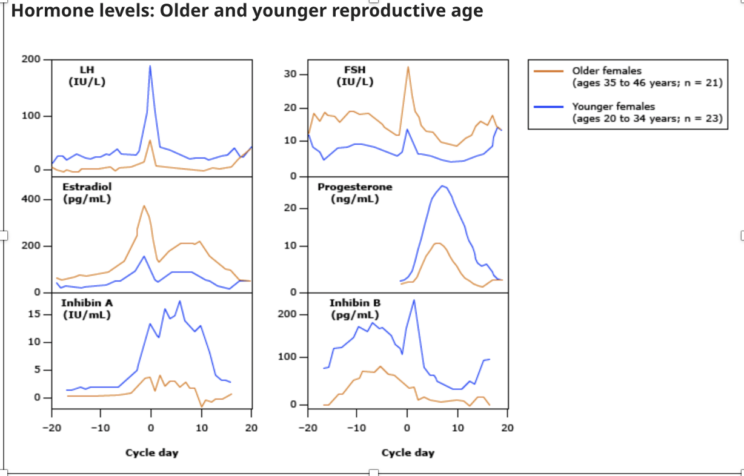
APPENDIX C : Hormone level changes with age
References:
ACOG Committee opinion 773 (reaffirmed 2020)
Yen and Jaffe’s Reproductive Endocrinology (2019), Ch: Ovarian life cycle